The DSM Scam
The Diagnostic and Statistical Manual of Mental 
The Diagnostic and Statistical Manual of Mental Disorders (DSM) of the American Psychiatric Association (APA) is the manual that provides a symptom list for diagnosing a catalogue of mental illnesses. The first edition DSM, published in 1952, was strongly influenced by Freudian thinking. It classified depression as a psychosis, either involutional melancholia or manic-depressive psychosis. Under this regime depression was a relatively rare event.
Mental Disease becomes a Mental Disorder
In the 1970s psychiatry was in a crisis because of uncertainty over what actually constituted mental illness. A big problem was that in the early DSM no mental illness met the definition of a disease. Psychiatry dealt with this problem by creating the category of ‘disorder’ as a rhetorical device. In this way of thinking, a mental ‘disorder’ is kind of like a disease, but it does not have all the characteristics of a disease, such as biological markers.[1] This rhetoric sleight of hand has allowed the DSM process to invent hundreds of mental ‘disorders’, which they treat like mental diseases, although they are not diseases.
Dr Robert Spitzer, professor of psychiatry at Columbia University, was the driving force behind DSM-III. He identified himself as an atheist and a secular humanist.[2] He took the job determined to create a whole new DSM that would eradicate human bias and Freudian obsessions with the ‘unconscious’. In the process he annoyed traditional psychoanalysts by removing the term ‘neurosis’ from the DSM.
DSM-III
Having recognised the problems with Freudian psychoanalysis, 
DSM-III created an entirely new way of looking at mental 
The publication of DSM-III in 1980 caused a sensation. All professionals in the mental health industry, social workers, psychologists, general practioners and even lawyers, wanted to read the new ‘bible’ of mental disorders. The new 567-page manual became an unlikely best seller. The APA released a revised version of the DSM-III in 1987. For the first time the name to attention deficit hyperactivity disorder (ADHD) appeared.
The list of symptoms for establishing a diagnosis of depression was constructed by the subjective opinions of Spitzer’s small group of psychiatrists and not on any objective scientific evidence.
Spitzer commented:
‘Our team was certainly not typical of the psychiatry community, and that was one of the major arguments against DSM-III: it allowed a small group with a particular view point to take over psychiatry and change it in a fundamental way…It was a revolution, that’s what it was. We took over because we had the power.’[3]
James Davies comments;
‘This powerful few had established for a whole new generation where the thin membrane separating psychiatric disorder from the ordinary troubles of life should be set. They had created and defined approximately 80 new mental disorders… And all the while, the truth about the processes going on behind the scenes remained carefully hidden; processes that have dramatically increased the number of us today being branded psychiatrically unwell.’[4]
And here we have uncovered the massive problem that lies behind the DSM fraudulent process—the DSM had not discovered mental disorders; it had created them.
The saga around homosexuality reveals much about the 
Here we see the power of the DSM to create a ‘mental illness’, and the power to remove a ‘mental illness’ from its catalogue of ‘disorders’; this is not science, this is political expediency.
DSM-IV
Dr Allen Frances was appointed Chairman of the DSM-IV 
The most important symptoms for a diagnosis of depression are (1) a depressed mood, and (2) markedly diminished interest or pleasure in most or all activities. Other symptoms are significant weight loss or weight gain; insomnia or hypersomnia; fatigue or loss of energy; feelings of worthlessness; excessive or inappropriate guilt; diminished ability to think or concentrate or indecisiveness.
Interviewed by James Davies, Allen Frances referred to three false 
‘We now have a rate of autism that is twenty times what it was fifteen years ago. By adding bipolar II we also doubled the ratio of bipolar versus unipolar depression, and that’s resulted in lots more use of antipsychotic and mood stabiliser drugs. We also have rates of ADHD that have tripled, partly because new drug treatments were released that were aggressively marketed.’
Among the weirdest disorders included in DSM-IV are: social phobia (shyness or fear of public speaking); reading disorder (falling substantially below the reading standard for age); non-compliance with treatment (patient persistently refuses recommended treatment); oppositional defiant disorder (children overtly defy authority).
DSM V
Published in 2013, DSM-V is an attempt to provide doctors with a definitive list of all recognised mental health conditions, including their symptoms. But DSM-V proved to be hugely controversial. The two main criticisms were, first, the unhealthy influence of the pharmaceutical industry. Links and potential conflict of 
Dr Allen Frances is highly critically of the latest update of the DSM. He comments:
‘DSM-V is proposing changes that will dramatically expand the realm of psychiatry and narrow the realm of normality – resulting in the conversion of millions more patients, millions more people, from currently being without mental disorders to be psychiatrically sick. What concerns me about this reckless expansion of the diagnostic boundaries is that it will have many unintended consequences, which will be very harmful… there is the new ‘generalised anxiety disorder’, which threatens to turn the aches and pains and disappointments of everyday life into mental illness. There is ‘minor neurocognitive disorder’ that will likely turn the normal forgetting of ageing into a mental illness. There is ‘disruptive mood dysregulation disorder’, which will see children’s temper tantrums become symptoms of disorder. The changes will expand the definition of mental illnesses to include more people, exposing more to potentially dangerous psychiatric medications.’[6]
And the criticism went further with articles in the Lancet and New England Journal of Medicine strongly criticising the DSM for turning grief into a mental disorder. The emotion of grief, once excluded from the definition of depression, is now included within it. This means that people grieving over the death of a loved one could go to their psychiatrist and be prescribed pills to treat what the DSM has labelled ‘prolonged grief disorder’ (PGD). Critics, writing in The Lancet, argue that the medicalization of grief is misguided, for it has increased the group of people to be treated with antidepressants.
Depression
A brochure produced by the American Psychiatric Association 
According to the National Institute of Mental Health there is no single known cause of depression. ‘Rather, it likely results from a combination of genetic, biochemical, environmental, and psychological factors. Research indicates that depressive illnesses are disorders of the brain… The parts of the brain responsible for regulating mood, thinking, sleep, appetite and behaviour appear to function abnormally. In addition, important neurotransmitters – chemicals that brain cells use to communicate – appear to be out of balance.’[9] So while the exact cause of depression is not known, the mental health profession claims that depression is due to abnormal brain function caused by an imbalance of brain chemicals. However, there is not a shred of evidence to support the theory of a chemical imbalance.
Note the highly subjective nature of the diagnosis. It depends entirely on what the patient tells the psychiatrist, who must use clinical judgment to decide whether the patient’s self-reported symptoms fulfil the diagnostic criteria to earn the label of depression. The diagnostic difficulties are not difficult to see. How many people suffer, from time to time, with fatigue, insomnia, indecisiveness or diminished interest in pleasures? And there’s another major problem – many people stand to benefit from a diagnosis of depression, for they are then considered to be sick and therefore not responsible for their behaviour. They may also be able to take time off work and even claim 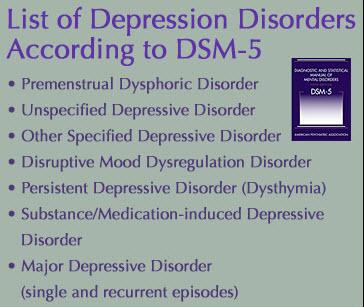
Another diagnostic difficulty is that clinicians vary in the way they interpret a patient’s symptoms. This means is that the diagnosis of depression is arbitrary and totally subjective. We must underline the fact that there are no clear, objective diagnostic criteria. There is no physical sign, blood test or X-Ray that can confirm the diagnosis. All depends on what the patient says and how the psychiatrist interprets the symptoms. Indeed, to distinguish between mood changes that all people experience as a part of the give and take of life and the mental disorder of depression is a very difficult task.
Professor of Psychiatry, Gordon Parker, in an article in the British Medical Journal argues that depression is being hopelessly over diagnosed. Parker says that a low threshold for diagnosing depression risks treating normal emotional states as illness.[10] Indeed, if ten per cent of the population suffers with depression (a serious medical illness) each year, as we are informed by the APA, over time almost the entire population will have suffered with a serious disorder of the brain.
In his book, Cracked: Why Psychiatry is Doing More Harm 
The above discussion shows how the DSM has opened the depression floodgate. Moreover, the subjective criteria for making a diagnosis of depression have been strongly influenced by psychiatrists that have a financial link to the pharmaceutical industry. By broadening the diagnostic criteria, the DSM has succeeded in creating a large market for anti-depressant drugs.
Biblical critique of DSM
The DSM, often referred to as the ‘bible’ of psychiatry, is the product of men devoid of spiritual understanding and grounded in the thinking and ways of the world. Sigmund Freud’s concept of the anxiety neurosis was a major organizing principle of the early DSM. An article in The New Yorker, entitled ‘Why Freud Survives’,[11] describes how during the 1930s and 40s about fifty Freudian psychoanalysts immigrated to the United States. ‘They were some of the biggest names in the field, and they took 
With his invention of the unconscious mind, Freud claimed to have uncovered the source of human emotional pain, which he also claimed could be alleviated through psychoanalysis, which delved into the unconscious. He taught that most neurotic behaviour was caused by repressed sexual desires, such as the Oedipus complex.
As the influence of Freud declined, the APA saw the need to refresh the DSM to make it more relevant. Along came Dr Robert Spitzer, who described himself as an atheist Jew and secular humanist, to update the flagging DSM. Spitzer’s DSM-III scrubbed out almost every trace of Freudianism as the concept of neurosis (which had lost credibility), was replaced with the concept of mental illness, caused by a disease of the brain, usually characterised by a chemical imbalance that could be cured by psychotropic drugs.
In the DSM we have a document that has been constructed entirely by human wisdom—there is no acknowledgement of divine wisdom, and no understanding that Scripture has much to say about the causes of human suffering and the need for spiritual salvation. The DSM does not recognise that man is a spiritual being, created in the image of God; it does not understand that faith in Christ brings the peace of God that surpasses all understanding, and guards the heart and mind of believers (Philippians 4.7).
Dr Ed Payne, editor of the Journal of Biblical Ethics in Medicine, makes the point that psychiatry, and thus the DSM, is rooted in secular humanism.
‘Sigmund Freud, Carl Jung, and other “fathers” were often avowed atheists. Their modern counterparts have continued this separation of religion, specifically Biblical Christianity, from psychiatry. A Christian with any understanding of spiritual issues should ask, “How can an understanding of the thinking and behaviour of man omit the record and explanations of Him who created, cursed, and saved mankind?” Any basic understanding of Christianity and philosophy reveals the incompatibility of concepts that grow out of secular humanism and Biblical truth. The war of these worldviews is seen in every area of society—sexual norms, alcoholism, addiction, marriage, child-rearing, abortion, euthanasia, in vitro fertilization, gun control, etc.’[12]
Dr Payne is drawing attention to the ideology that underpins the DSM—secular humanism.
What Freud and Spitzer have in common is that they are both men who have no knowledge of the spiritual nature of man. Both set themselves up as prophets who have the answer to human emotional suffering. Neither of them understood that human nature is sinful, and that sin has a powerful effect on the human condition. Neither acknowledged that God has spoken through His Word—the Bible. Like the Pharisees of biblical times, they followed the traditions and thinking of men, and denied the wisdom of Christ. They have no understanding that the real problems of man reside in the sinful heart of man. That all have sinned, and that the wages of sin is spiritual death; that there is no rest for the wicked. They do not accept that sin causes fear, shame and guilt. A crucial point that they miss entirely is that much of what they have labelled as mental illness is, in fact, the result of human sin.
The precepts of men
The Bible gives the strongest possible warning that we should not place our trust in the precepts and ideas of man, such as the DSM. ‘Thus says the Lord: “Cursed is the man who trusts in man, and makes flesh his strength, whose heart departs from the Lord”.’ (Jeremiah 17.5).
Scripture exhorts us to not place our trust in the precepts of man, and especially not in the precepts devised by powerful people. ‘Do not put your trust in princes, nor in a son of man, in whom there is no salvation’ (Psalm 146.3). And: ‘It is better to trust in the Lord, than to put confidence in man. It is better to trust in the Lord, than to put confidence in princes’ (Psalm 118.8-9, NKJV). And again, ‘Through thy precepts I get understanding: therefore I hate every false way’ (Psalm 119.104).
Throughout the Bible we are warned to not place our trust in the thinking and precepts of man. This means that a faithful Christian cannot accept the ungodly wisdom of the DSM. Scripture warns of a way that seems right to man, but the end thereof is the way of death (Proverbs 14.12). The way that seems right is the way of the fool who has no fear of God before his eyes. We must not lean on our own understanding (Proverbs 3.5); we must not place our trust in the precepts of the princes of psychiatry, who in defiance of biblical truth, have arrogantly set themselves up as experts in human behaviour.
Two new mental disorders created by DSM-IV – ‘conduct disorder’ and ‘antisocial personality disorder (ASPD)’ – illustrate the secular, godless mindset that drives the world of the DSM.
Conduct disorder
Children and adolescents with ‘conduct disorder’, according to DSM-IV, ‘may display bullying, threatening, or intimidating behaviour; initiate frequent physical fights; use a weapon that can cause serious physical harm (e.g. a bat, brick, broken bottle, knife, or gun); be physically cruel to people or animals; steal while confronting a victim (e.g. mugging, purse snatching, extortion or armed robbery); or force someone into sexual activity; physical violence may take the form of rape, assault, or in rare cases, homicide.’[13] In effect, the DSM is asserting that those who lie, steal, rape and murder are mentally ill, and therefore not responsible for their actions. It is entirely oblivious that it is describing sinful behaviour as mental illness.
Antisocial personality disorder (ASPD)
A well referenced Wikipedia article gives the following definition. ‘Antisocial personality disorder is defined by a pervasive and persistent disregard for morals, social norms, and the rights and feelings of others. Individuals will typically have no compunction in exploiting others in harmful ways for their own gain or pleasure and frequently manipulate and deceive other people, achieving this through wit and a façade of superficial charm or through intimidation and violence.’
Scripture does not see the actions and attitudes that DSM-IV has chosen to label ‘conduct disorder’ and ‘antisocial personality disorder’ as features of a mental illness. On the contrary, Scripture teaches that lying, stealing, violence, disobedience, rebellion, anger, rape and murder are sinful actions condemned by God’s law—the fruit of an evil, wicked, rebellious heart. Jesus said, ‘For from within, out of the heart of men, proceed evil thoughts, adulteries, fornications, murders, thefts, covetousness, wickedness, deceit, lewdness, an evil eye, blasphemy, pride, foolishness. All these evil things come from within and defile a man’ (Mark 7:21-23).
The Christian Faith offers hope to those who are slaves of sin, given over to every kind of immoral conduct. They need to hear the gospel of salvation. The answer to their sinful lifestyle is and turn toward God in repentance and to place their faith in our Lord Jesus Christ (Acts 20.21). ‘If anyone is in Christ, he is a new creation; old things have passed away; behold, all things have become new’ (2 Corinthians 5.17).
What we have uncovered is a fundamental difference in the way the DSM, on the one hand, and Scripture, on the other hand, view the nature of man’s problem. The DSM, from its stance in secular humanism, does not recognise the spiritual nature of man and has no understanding of the nature and consequences of sin. It seeks to persuade society that the people it labels with ‘depression’, ‘conduct disorder’ or ‘oppositional defiant disorder’ are suffering with a disorder of the brain and therefore not responsible for their actions and in need of psychiatric help.
Conclusion
The DSM is a gigantic fraud that is being perpetrated on human kind by the psychiatric profession. Because the DSM is unable to define mental illness, it has coined the vague word ‘disorder’ to describe the conditions over which psychiatry exerts control. During the past five decades the DSM has invented a catalogue of hundreds of mental ‘disorders’ that medicalize life. Even grief following bereavement has been turned into ‘prolonged grief disorder’. The concept of ‘disorder’ gives to the princes of psychiatry the power to create conditions that need psychotropic drugs. The scam of the DSM is that it has taken to itself the power to create a ‘mental disorder’ by the majority vote of a small group of psychiatrists, most of whom are linked to Big Pharma. It goes without saying that there is no biological marker to confirm the diagnosis of such a ‘disorder’. Depressive disorders are the most common condition created by the DSM. All that is needed for a diagnosis of depression is the subjective opinion of a psychiatrist, who follows a checklist of symptoms. This laxity in diagnosis has led to an epidemic of depression in the USA and UK, and in many other countries around the world, as around 1 in 4 people have a lifetime chance of receiving a diagnosis that can lead to a lifetime on antidepressant drugs. The greatest achievement of the DSM scam has been to legitimise the prescribing of mind-altering drugs to millions of people. The DSM stands guilty of ‘biblical defiant disorder’.
Endnotes
[1] The Real Problems with Psychiatry, A psychotherapist contends that the DSM, psychiatry’s “bible” that defines all mental illness, is not scientific but a product of unscrupulous politics and bureaucracy, by Hope Reese, May 2, 2013: https://www.theatlantic.com/health/archive/2013/05/the-real-problems-with-psychiatry/275371/
[2] Christianity Today, May (Web-only) 2001, Vol. 45, Gays can change says Columbian University Professor’s study
[3] James Davies, Cracked (2013), pp34-35
[4] Cracked, p35
[5] Cracked, p14-15
[6] Cracked, pp52-53
[7] American Psychiatric Association, ‘Let’s talk about depression’, website.healthyminds.org
[8] Article in Pulse, ‘Antidepressant prescriptions increased by half a million last year’, 24 July 2018, by Elisabeth Mahase: http://www.pulsetoday.co.uk/clinical/clinical-specialties/prescribing/antidepressant-prescriptions-increased-by-half-a-million-last-year/20037121.article
[9] National Institute of Mental Health, website, www.nimh.nih.gov/health/publications/depression/
[10] Gordon Parker, Is depression over diagnosed? Brit Med Jour, 18 August 2007, volume 335, p328
[11] The New Yorker, A Critic at Large, August 28, 2017 Issue; ‘Why Freud Survives, He’s been debunked again and again—and yet we still can’t give him up’ by Louis Menand, https://www.newyorker.com/magazine/2017/08/28/why-freud-survives
[12] The Bible vs. DSM-IV in ‘Biblical Reflections on Modern Medicine’, Vol. 10, No. 4 (58), editor Dr Ed Payne
[13] Diagnostic and Statistical Manual of Mental Disorders (DSM-VI), Fourth edition, text revision, American Psychiatric Association, 2004, p94



No comments:
Post a Comment